President Donald J. Trump & Secretary Robert F. Kennedy Jr.
On Winning 2026 — MAHA and the Politics of Delivery
May 2026 · greathealthalliance.org
I.
The Mandate Is Real — and Bipartisan
A national survey provides the empirical foundation for everything that follows. Methodology: stratified sampling by past election turnout, mixed-mode interviewing. The findings are directionally reliable and have since been corroborated by the KFF April 2026 Health Tracking Poll.
The headline finding is not that health issues poll well with MAHA voters. It is that they poll well with everyone.
Figure 1
Bipartisan Health Concerns — % of Registered Voters
Issue / Statement
% Concerned / Agree
Pharma industry influence in public policy
90% / +82 Net
Obesity, including childhood obesity
90% / +81 Net
Toxic chemicals in agriculture
89% / +80 Net
Cheaply produced and unhealthy foods
88% / +79 Net
Unaffordable healthy foods
88% / +77 Net
Ultra-processed foods
85% / +74 Net
Regulate chemicals banned in Europe
89% Agree
Healthy food in school lunches & food stamps
87% Agree
Combat corporate capture in medicine
86% Agree
FDA limit harmful chemicals in food
67% Agree
Shift healthcare budget to healthier food
60% Favor
Source: National RV Survey. n=1,500 registered voters.
Pharma distrust scores +82 net overall — +85 Republican, +84 Independent, +77 Democrat. That is not a partisan finding. The mandate to act on food safety, chemical regulation, and healthcare corruption does not require coalition-building. The coalition already exists.
II.
The Snapshot and the Direction
The survey shows a 54/45 split on overall vaccine safety concern — 54% not concerned, 45% concerned. In isolation this appears to favor the status quo. In historical context it is a seismic shift.
A Note on Directionality
Five years ago, a 45% vaccine concern figure among registered voters would have been unthinkable. The COVID vaccine rollout, the mandates, the suppression of adverse event reporting, and the slow emergence of myocarditis findings have moved this number dramatically.
The snapshot shows a movement consolidating its base. The direction shows a public still in motion. The thin social-pressure layer that maintains the "safe and effective" consensus as a label — even as its institutional foundations erode — is not a stable equilibrium. It is a waystation.
The vaccine-adjacent findings confirm the pattern:
74%
Oppose Blanket Pharma Immunity
68%
Want NIH to Redo Vaccine Research
58%
Want Infant Schedule Studied
45%
Favor Family Vaccine Choice
74% of all voters oppose blanket immunity for vaccine manufacturers. This question would have been fringe to even ask in 2019.
68% want NIH to redo vaccine safety research. 51% of Democrats agree.
58% say NIH should study complications from infants receiving too many vaccines too quickly.
45% want families to choose their own vaccination timeline. Only 8% say vaccines are outright unsafe.
The 8% figure is the key. The public is not anti-vaccine. They are anti-impunity, anti-coercion, and anti-capture. The winning frame is accountability and transparency — not vaccine danger. That frame captures the 42% persuadable "concerned but not MAHA-identified" bloc without triggering the anti-science response that loses them.
Source: National RV Survey.
III.
The Swing Vote Equation: MAHA Is the Margin
President Trump won the 2024 election by 2.3 million popular votes. He won Wisconsin by fewer than 30,000 votes. Had Harris carried Michigan, Wisconsin, and Pennsylvania — which Trump won by a combined 230,000 votes — she would have won the Electoral College.
Robert F. Kennedy Jr. was polling 3–6% at his peak, representing an estimated 4.5–9 million motivated voters. Pre-election research found that among swing voters in a six-way race, Kennedy drew 46% support. After his endorsement of Trump and withdrawal, a substantial portion moved to Trump.
Sources: Data for Progress, "Measuring the Swing," May 2024; Pew Research Center, "The Presidential Choice: Biden, Trump, Kennedy," July 2024; Divided We Fall, "Did RFK Jr. Reshape the 2024 Election?," August 2024.
These were not generic protest voters. They were single-issue motivated on pharma accountability, food safety, and vaccine choice. They crossed party lines deliberately and have no party loyalty to fall back on. The commitment that brought them was specific: that someone in government would finally fight the captured institutions that had damaged their families.
The Republican Party is renting MAHA voters. They haven't decided to purchase them yet.
MAHA Action Memo to Republican Campaign Chairs · February 2026
The MAHA PAC has quantified this explicitly: MAHA voters could represent 10% of the electorate, and Republican candidates must give them a concrete reason to turn out. Meanwhile, one in three MAHA supporters currently disapprove of Kennedy's job performance — not because he has gone too far, but because tangible change has not matched the promise.
Sources: Axios, "RFK Jr.'s MAHA movement becomes wild card for GOP in 2026 midterms," February 13, 2026; KFF Quick Takes, "Secretary Kennedy Remains Popular with MAGA and MAHA Supporters, But Few Others," April 2026.
The Conventional Wisdom and Its Limits
The standard inner-circle argument: vaccines are a losing issue, suburban moderates are alienated, the generic ballot favors Democrats by five points — therefore soften, triangulate, chase the middle. This argument fails on three grounds.
The middle does not reward the concession. The 42% "concerned but not MAHA-identified" bloc views Trump unfavorably by 47 points. They are reachable on food, pharma, and costs — not on cultural concessions.
The base is not replaceable. MAHA voters are grievance-motivated: personal stakes produce outsized turnout and volunteer energy that do not appear in preference polling but appear in November.
The leading vulnerability is accountability failure, not vaccine skepticism. The April 2026 Data for Progress poll found the most effective attack is Kennedy's "failure to stand up to Big Pharma and lower costs." That is the base's complaint too. The answer is not retreat — it is delivery.
Secretary Kennedy's first year has been genuinely transformative by any historical standard:
Updated Dietary Guidelines 2025–2030 emphasizing whole foods and full-fat dairy
ACIP reconstituted with vaccine skeptics; childhood immunization schedule under active review
$500 million in mRNA vaccine development contracts terminated
CDC website updated to acknowledge vaccine-autism link as an open research question
New research funded on autism, Lyme disease, and food additives
MAHA branding extended across EPA, Transportation, and Agriculture
Sources: The Hill, February 13, 2026; PBS NewsHour, January 2, 2026; STAT News, December 17, 2025.
And yet: KFF April 2026 finds only one in three MAHA supporters strongly approve of the administration's health handling. Awareness has outpaced delivery. Movement has outpaced governance.
The Structural Gap
Executive and regulatory action can change guidelines, restructure panels, fund research, and shift recommendations. It cannot do the one thing voters list as their primary concern: reduce healthcare costs.
Healthcare costs are cited by 55% of voters as a major factor in their 2026 vote — 15 points higher than food safety or vaccine policy. This is the central terrain of the midterm election, and executive action alone cannot hold it.
The Base Wants Costs Too
The May 2026 KFF Health Tracking Poll surfaces a finding that changes the strategic calculus: among MAHA-aligned voters themselves, 42% rank healthcare costs as their #1 federal health priority — compared to just 21% for food additives and 10% for vaccines.
This is not a case of soothing the persuadable middle by softening MAHA priorities. The MAHA base is itself asking for cost relief — by a four-to-one margin over the next priority. Costs are not a concession. They are the convergence point where the base and the swing voter meet.
A national survey of 1,600 likely voters conducted January 22–25, 2026 by McLaughlin & Associates for the Great American Health Alliance — margin of error ±2.5%, demographics reflecting a 2026 general election turnout model — settled the policy question before this letter was written. The American electorate is not waiting to be persuaded. The mandate already exists.
79%
Say the system faces a crisis or major problems
81%
Tired of "sick care" — want wellness investment
76%
Have intense concerns about out-of-pocket costs
85%
Want real price & coverage transparency
The findings line up with the directional logic of this entire letter. Four out of five voters reject the status quo. Four out of five want a system built around wellness rather than sickness. Three-quarters want greater control over their own health dollars. None of this is contested terrain.
The "Renting vs. Owning" Frame Already Polls
Paying monthly health insurance premiums feels like renting my coverage — I build no equity or long-term value and it all goes away if I can't pay for it anymore or switch insurers.
79% Agree · McLaughlin / GAHA National Survey · January 2026
This is the ownership-economy argument applied to healthcare — and 79% of likely voters already agree with it without having heard it from any political leader. It is also, by remarkable coincidence, the structural mirror of the MAHA Action memo's warning that "the Republican Party is renting MAHA voters." Both the policy and the politics fail for the same reason: renting builds no equity. Ownership does.
Healthier Spending Accounts — The Coalition Already Built
The McLaughlin poll tested the GAHA framework directly. Voters were presented with the Healthier Spending Account concept — annual federal deposits into personal accounts owned by the individual, portable for life, usable for medical care, wellness, fitness, mental health, nutritional supplements, and preventive measures. The response is the most decisive finding in the survey.
Figure 2
Bipartisan Support for Healthier Spending Accounts
Voter Group
% Support / Oppose
All Likely Voters
73% / 17%
Republicans
82% / 10%
Democrats
66% / 24%
Independents
70% / 17%
White voters
74% / 16%
Hispanic voters
73% / 16%
Black voters
73% / 19%
Voters 18–34
76% / 17%
Voters 65+
72% / 17%
Source: McLaughlin & Associates / Great American Health Alliance, January 22–25, 2026. n=1,600 likely voters, ±2.5% MOE.
Read those numbers again. There is no demographic in which support drops below 66%. There is no racial group with less than 73% support. There is no age cohort below 72%. This is not a partisan policy with an upside. It is a near-consensus policy with congressional inertia as its only meaningful opposition.
The Specific Features Poll Even Higher
When the survey moved from the general concept to specific design features, support climbed further:
86% support unused dollars rolling over and growing tax-free for life.
86% support spending health dollars on doctors, dentists, optometrists, procedures, and prescription medicines.
85% support full portability — the account stays with the individual for life.
82% support total personal control without government or insurance interference.
80% support using health dollars on gym memberships, fitness, mental health, over-the-counter medicines, vitamins, and nutritional programs — the precise MAHA coverage agenda.
76% support the federal government depositing health dollars directly into personal accounts instead of sending money to insurers.
That last figure is the political earthquake. 76% of likely voters want the federal government to bypass insurance companies entirely and pay individuals directly. This is structural reform with overwhelming public consent already in hand.
The Electoral Multiplier
The survey did not stop at policy preference. It tested electoral consequences directly:
67%
More likely to vote for a congressional candidate who supports HSAs
77%
Republicans more likely to vote for HSA supporter
60%
Democrats more likely to vote for HSA supporter
62%
Independents more likely to vote for HSA supporter
Two-thirds of likely voters say they would be more likely to vote for a congressional candidate who supports Healthier Spending Accounts. This crosses every partisan line. It crosses every demographic — 74% of voters 18–34, 73% of Black voters, 72% of Hispanic voters. The political upside is not theoretical. It is documented, polled, and waiting to be claimed by whoever moves first.
A Note on Methodology
This survey was commissioned by the Great American Health Alliance and conducted by McLaughlin & Associates, a Republican-aligned polling firm with established national methodology. Both facts should be on the table. Sponsored polling is a legitimate part of policy advocacy when methodology is transparent and findings are presented honestly. The standard test for such polling is replicability — and these findings are consistent with the independent KFF Health Tracking Polls of April and May 2026 on healthcare cost concern, with the directional public mood captured by independent national surveys of registered voters, and with the GOP's own internal urgency reflected in the MAHA Action memo. The methodology holds. The numbers are what they are.
The implication for the inner circle is direct. Every other policy debated for the midterms requires building a coalition that does not yet exist. The Healthier Spending Account coalition already exists, and it is overwhelming. The only remaining variable is whether congressional Republicans choose to claim it before Democrats find a way to copy it.
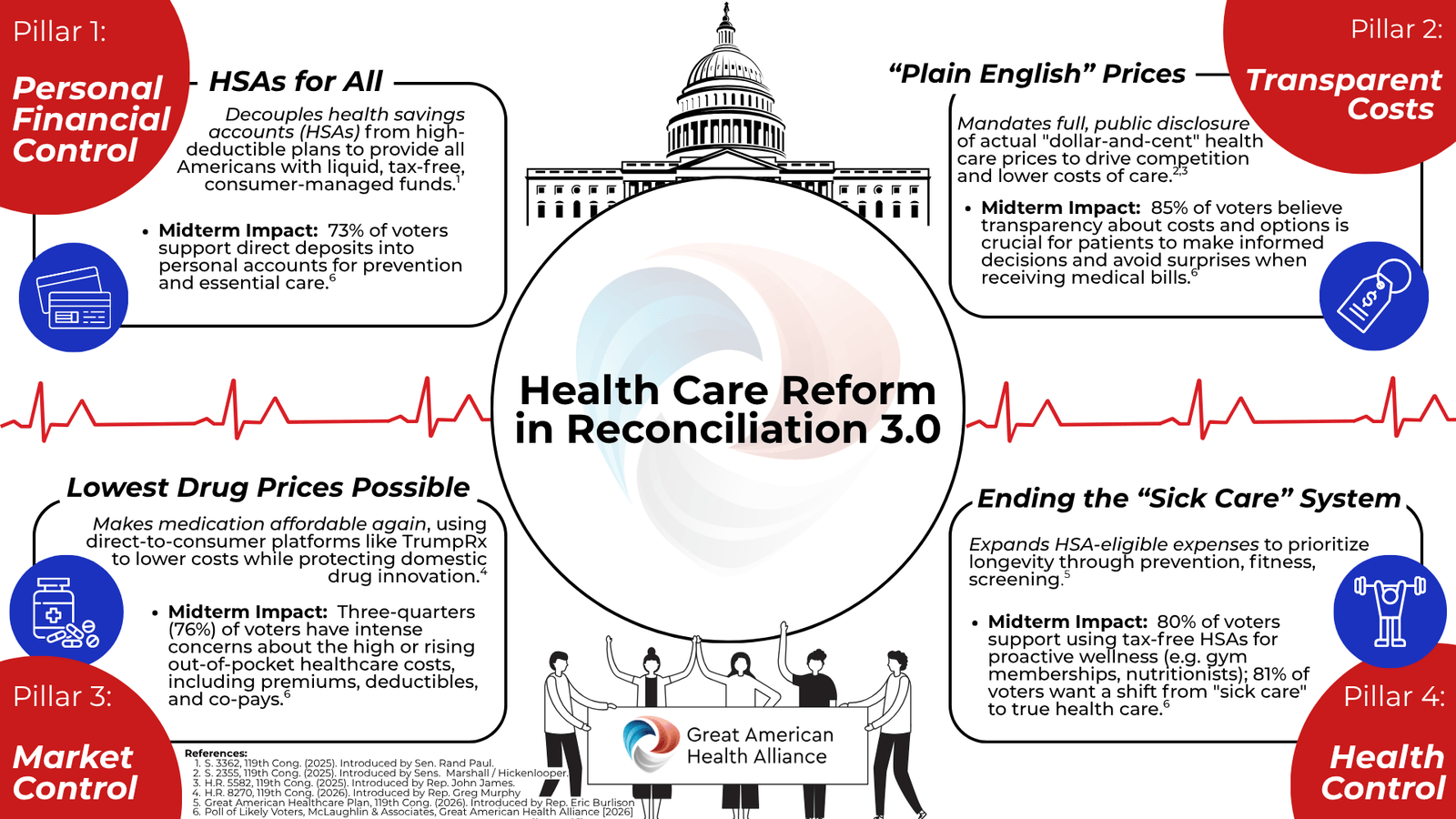
The Four Pillars — Health Care Reform in Reconciliation 3.0
The Great American Health Alliance has organized the legislative agenda around four structural pillars, each linked to specific bills already introduced in the 119th Congress and each backed by majority public support. This is not a policy wish list. It is a complete architecture for reform, with sponsors, bill numbers, and polling already in hand.
GAHA has published this architecture as the Reconciliation 3.0 Legislative Roadmap:
Decouples health savings accounts from high-deductible plans to provide all Americans with liquid, tax-free, consumer-managed funds.
Midterm Impact73% of voters support direct deposits into personal accounts for prevention and essential care.
S. 3362, 119th Cong. (2025) — Sen. Rand Paul (R-KY)
Pillar 2 · Transparent Costs
"Plain English" Prices
Mandates full, public disclosure of actual dollar-and-cent health care prices to drive competition and lower costs of care.
Midterm Impact85% of voters believe transparency about costs and options is crucial for patients to make informed decisions and avoid surprises when receiving medical bills.
S. 2355, 119th Cong. (2025) — Sens. Marshall / Hickenlooper · H.R. 5582, 119th Cong. (2025) — Rep. John James
Pillar 3 · Market Control
Lowest Drug Prices Possible
Makes medication affordable again, using direct-to-consumer platforms like TrumpRx to lower costs while protecting domestic drug innovation.
Midterm ImpactThree-quarters (76%) of voters have intense concerns about high or rising out-of-pocket healthcare costs, including premiums, deductibles, and co-pays.
Expands HSA-eligible expenses to prioritize longevity through prevention, fitness, and screening.
Midterm Impact80% of voters support using tax-free HSAs for proactive wellness (gym memberships, nutritionists); 81% want a shift from "sick care" to true health care.
H.R. 8324, 119th Cong. (2026) — Rep. Eric Burlison (R-MO) — Great American Healthcare Plan
Each pillar maps to legislation already introduced. Each pillar maps to polling already conducted. The architecture is complete. The question for congressional leadership is no longer what to pass — it is the order of operations and the calendar.
The Burlison Great American Healthcare Plan integrates Pillars 1 and 4 into the most ambitious vehicle. The Paul HSA bill provides the foundational reform. The Marshall–Hickenlooper transparency bill is the rare bipartisan healthcare instrument. The Murphy bill addresses the drug pricing concern that polls highest among midterm voters. Bundled into a reconciliation package, these four pillars would constitute the most consequential domestic policy achievement of the Trump administration's second term — and the most durable.
Sources: S. 3362 (Paul); S. 2355 (Marshall/Hickenlooper); H.R. 5582 (James); H.R. 8270 (Murphy); Great American Healthcare Plan (Burlison); Polling: McLaughlin & Associates / Great American Health Alliance National Survey of 1,600 Likely Voters, January 22–25, 2026.
VII.
GAHA — The Legislative Bridge, Already Introduced
The Great American Health Alliance is the legislative complement to MAHA's executive track. Where MAHA operates inside the regulatory apparatus, GAHA operates in Congress. Where MAHA shifts guidelines, GAHA changes law. Where MAHA can be reversed by the next administration, GAHA cannot.
The Bill Is on the Floor
On April 16, 2026, Rep. Eric Burlison (R-MO) introduced H.R. 8324 — the Great American Healthcare Plan — a patient-first, cost-lowering package centered on Health Savings Account expansion, price transparency, competition, and direct consumer control. The bill codifies the Trump administration's January 2026 "Great Healthcare Plan" and is backed by the Great American Health Alliance coalition pushing it as the vehicle to codify MAHA priorities permanently.
The argument is no longer hypothetical. The legislation exists. The coalition exists. The White House framing exists. What remains is the political will to pass it before November.
The core instrument is the Great American Health Plan: a universal Health Savings Account framework incorporating a MAHA-curated list of covered products and services. Earlier 2025 reconciliation legislation already expanded HSA eligibility to Bronze and Catastrophic plans and direct primary care arrangements — building the foundation. The Burlison bill carries that foundation forward into a universal framework. The contents are the MAHA agenda: integrative practitioners, autism and vaccine injury therapeutics, advanced diagnostics, environmental health products, and compounded medications.
What GAHA Adds
Healthcare Cost Relief — the #1 Voter Concern
Universal HSAs directly address affordability by allowing Americans to pay for health services — including MAHA-aligned preventive and integrative care — with pre-tax dollars, without insurance gatekeeping. This is tangible, personal, immediate cost relief. It answers the question 55% of voters say will determine their November vote.
Delivery That Can Be Pointed To
Democrats lead Republicans on healthcare trust by double digits (41% vs. 25%, KFF April 2026). GAHA closes that gap with a concrete answer: we passed a law. No administration can undo it. Every American who uses an HSA for a naturopath visit, a child's autism therapeutic, or a compounded medication is living proof of delivery.
Bipartisan Legislative Surface Area
HSA expansion has Republican DNA. It can pass with Republican votes alone. The MAHA coverage list inside it delivers to the base through a vehicle Congress can accept. The wrapper passes. The contents honor the coalition.
Permanence
Every executive action Kennedy has taken can be reversed by his successor. Legislation requires a congressional majority to undo. GAHA codifies MAHA permanently.
The Answer to the Credibility Attack
The leading Democratic attack for 2026 is already visible: Kennedy has cut Medicaid and medical research, upended vaccine guidance, and failed to stand up to Big Pharma. The answer to this attack is not messaging. It is legislation. GAHA transforms the argument from "trust us" to "here is the law we passed."
VIII.
Tensions Acknowledged
The Vaccine Liability Argument
The April 2026 314 Action poll found RFK Jr.'s favorability drops 17 points among Independents and 18 points among soft MAHA voters after they learn his specific actions. This is a real finding.
The vulnerability is the perception of chaos and absence of tangible benefit — not vaccine skepticism per se. GAHA addresses this by replacing the narrative of disruption with delivery. HSA coverage for autism and vaccine injury therapeutics delivers to the injured without requiring the administration to litigate vaccine science in campaign ads.
The Donor Problem
Pharmaceutical industry donors have access that injured voters do not. Pressure to soften is real and should be named.
The political cost of pharma capture is now quantifiable. The MAHA Action memo has already done this work. If softening terms include pharma accountability, voters will notice. The mathematical consequence is demonstrated above.
The Generic Ballot
The generic congressional ballot favored Democrats by five points in October 2025. Trump's approval was -8. These are not favorable midterm conditions.
Generic ballot numbers at this stage are indicators, not determinants. 2024 was won against similar headwinds by assembling a non-traditional coalition. Losing the MAHA-Kennedy bloc is a concrete quantifiable risk. Retaining them through legislative accomplishment is a concrete quantifiable opportunity.
The Science Credibility Question
12% of voters who have heard MAHA recall it as "not based on science / misinformation." Among Democrats, 22%. The May 2025 MAHA Commission report was criticized for citations to non-existent studies.
The food safety, pharma accountability, and chemical regulation agenda is fully defensible scientifically — the 86–89% consensus confirms it. Lead with defensible science. Let the NIH vaccine research mandate stand on procedural merits: transparency and rigor, not predetermined conclusions. Avoid unforced errors.
IX.
Recommendations
Hold the Base First
Do not triangulate away from the MAHA-Kennedy coalition. The 4.5–9 million Kennedy voters who crossed party lines are the margin of victory. They are irreplaceable. The middle will not reciprocate the concession — but the base will notice the betrayal and stay home.
Lead With Pharma Accountability and Costs
The winning frame for 2026 is corporate capture and healthcare costs. Pharma distrust scores +82 net — +77 among Democrats. Healthcare costs, cited by 55% as a major midterm factor, must be answered with legislation, not messaging.
Pass the Burlison Great American Healthcare Plan
The Great American Healthcare Plan (H.R. 8324, Burlison, April 16, 2026) is already introduced and aligned with the White House's January 2026 healthcare announcement. Instruct congressional leadership to advance it through committee, layer in the MAHA-curated HSA coverage framework, and pass it before the August recess. This addresses the top voter concern, delivers to the base, closes the Democratic credibility gap on healthcare, and codifies the MAHA agenda against future reversal. The bill is on the floor. What remains is the political will to move it.
Honor the Injured
The vaccine-injured, the chronically ill, and the gaslit families are the moral core and motivational engine of this coalition. HSA coverage for autism therapeutics and vaccine injury services delivers to them tangibly. They will turn out. The persuadable middle may not.
Make the Math Visible to the Inner Circle
The argument most likely to move the President is numerical, not ideological. The Kennedy voter pool dwarfs the victory margin. Losing those voters through failure to deliver is the highest-probability path to losing the House. This report, or a condensed version, should reach the political team with the electoral arithmetic front and center.
Conclusion
The Case for Delivery
The MAHA movement has achieved something genuinely rare: it has moved the center of gravity on public health from institutional authority to personal accountability. The directional data confirms this is not a peak — it is a trend. The bipartisan mandate on food, chemicals, and pharma accountability is documented and durable. The voter coalition that delivered 2024 is watching for proof.
The risk is not going too far on accountability. The risk is not going far enough on visible, popular issues — food dyes, dietary guidelines, school lunches — while quietly retreating on the harder questions that motivated the base: who is liable, who captured the agencies, who suppressed the data, and what are we going to do about the children who were harmed.
MAHA answers those questions with executive authority. GAHA answers them with law. Together they close the gap between movement and governance, between motivation and delivery, between what was promised and what can be proven.
The voters who built this majority are not asking for perfection. They are asking for proof that someone is still fighting. The Great American Health Plan is that proof — written into statute, unreachable by the next administration, and visible to every American who opens their HSA and finds their naturopath, their child's autism therapist, their continuous glucose monitor, and their compounded medication finally covered.
The question is not whether to honor the commitment.The question is whether to do it before or after the election.The data suggests failure to deliver is more risky than playing to snapshot polls that don't factor the way the wind is blowing.
Sources & References
The Documentary Record
National Survey of 1,500 Registered Voters; October 2025. ±2.5% MOE.
Great American Health Alliance. "Health Care Reform in Reconciliation 3.0" (Four Pillars policy brief), 2026. greathealthalliance.org
S. 3362, 119th Congress (2025). HSAs for All. Introduced by Sen. Rand Paul (R-KY).
S. 2355, 119th Congress (2025). Healthcare price transparency. Introduced by Sens. Marshall & Hickenlooper.
H.R. 5582, 119th Congress (2025). Healthcare price transparency. Introduced by Rep. John James.
H.R. 8270, 119th Congress (2026). Drug pricing reform. Introduced by Rep. Greg Murphy (R-NC).
McLaughlin & Associates / Great American Health Alliance. National Survey of 1,600 Likely Voters. January 22–25, 2026. ±2.5%. greathealthalliance.org
H.R. 8324, 119th Congress (2026). Great American Healthcare Plan. Introduced by Rep. Eric Burlison (R-MO), April 16, 2026. Bill text: congress.gov · Press release: burlison.house.gov
The White House. "The Great Healthcare Plan." January 2026. whitehouse.gov
MAHA Action memo to Republican campaign chairs, Feb. 2026 (reported by Axios).